MUSCULAR DYSTROPHY; HOPE IN HEALING WITH AYURVEDA!

Muscular Dystrophy(MD) is a group of inherited genetic disorders that causes progressive muscle weakness and degeneration. Mutations in the genes that control the composition and functionality of muscle proteins cause it. Muscle wastage, loss of function, and difficulties affecting breathing, mobility, and even cardiac function are all common in people with muscular dystrophy.
In Ayurveda, this condition can be correlated to Mamsadhathu Kshaya(muscle tissue depletion) and Dhatu Agnimandya(Impaired metabolic function of tissue), primarily involving an imbalance in Vata Dosha. Specifically, it aligns with conditions like;
- Mamsa Kshaya: Due to improper nourishment of the muscle tissue, progressive muscle wasting occurs.
- Vata Vyadhi: Aggravated Vata Dosha(Neuromuscular Disorders) leads to muscle stiffness, weakness, and atrophy.
- Beeja Dosha(Genetic Defect): Ayurveda recognizes congenital and hereditary disorders caused by Beeja Dushti.
CAUSES OF MUSCULAR DYSTROPHY:
1. Genetic Mutations:
It is primarily caused by inherited genetic mutations affecting muscle proteins. These mutations can be;
- X Linked recessive: Passed to sons from mothers, affects usually males. Eg: Duchenne and Becker MD.
- Autosomal Recessive: It requires both parents to pass the defective gene. E.g.: Limb girdle MD.
- Autosomal Dominant: The defective gene from any parent can cause the disease. E.g.: Myotonic MD.
2. Insufficient Dystrophin protein:
- Dystrophin is crucial to maintain muscle integrity. Eg: Dystrophin is completely absent in Duchenne MD, whereas it is defective in Becker MD.
TYPES OF MUSCULAR DYSTROPHY(MD):
There are more than 30 different types of muscular dystrophy, but the most common ones include:
1.Duchenne Muscular Dystrophy(DMD):
- The most severe and prevalent type primarily affects men (females are typically carriers).
- Early childhood is when symptoms first manifest (2–5 years).
- The dystrophin protein, which is necessary for muscle stability, is absent due to a mutation in the dystrophin gene (DMD gene) found on the X chromosome.
CLINICAL FEATURES:
Early signs(Toddler to Early childhood):
- Motor milestones get delayed (like difficulty running, or late walking).
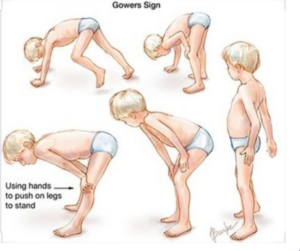
- Gower’s sign: Having trouble getting off the ground and having to push on thighs with the hands to get up.
- Falling frequently.
Child(5-12 years):
- Stair climbing is difficult.
- Weakness in the muscles of the thighs and hips.
- Waddling gait.
- It becomes difficult to do everyday tasks.
Adolescence(Teen years):
- Progressive loss of arm and leg muscular mass.
- Loss of walking abilities.
- Scoliosis
- Breathing problems brought on by respiratory muscle weakness.
Adulthood(Late teen to 20s-30s):
- Severe respiratory and cardiac problems.
- Weakening of the heart vessels, or cardiomyopathy.
- Ventilator support is required.
- Typically, people live for 20 to 30 years.
Prognosis:
- By their early teens, most kids are no longer able to walk.
- Respiratory and cardiac issues are prevalent in the late teens and early twenties.
- It is possible to live into your 30s or 40s with better care.
2.Becker Muscular Dystrophy(BMD):
A mutation in the dystrophin gene on the X chromosome causes Becker muscular dystrophy (BMD), a milder form of DMD in which some functional dystrophin is still generated.
CLINICAL FEATURES:
- Early adulthood to late childhood (5–30 years) is when it begins.
- Affected muscle groups: Likewise DMD, but progressing more slowly.
Key Symptoms:
- Initially, shoulder, thigh, and hip muscles are affected by muscle weakness.
- Delayed walking, while many people continue to be functional in adulthood.
- Frequent falls.
- Later on, Gower’s sign appears.
- Cramping in the legs.
Genetic cause and inheritance:
- Gene: X-linked recessive DMD gene.
- X-linked inheritance that mostly affects men.
Prognosis:
- Individuals maintain mobility into mid-adulthood.
- Although they happen later than in DMD, cardiac problems are common.
- With proper care, life expectancy can vary and frequently reach middle age or beyond.
3.Myotonic Dystrophy(DM)-Steinert’s Disease:
The most prevalent muscle dystrophy with an adult-onset is myotonic dystrophy (DM). It is a multisystem condition that affects the endocrine system, muscles, heart, and eyes.
Types:
- DM1(Classic Type): Caused by CTG repeat expansion in the DMPK gene.
- DM2(Milder Type): Caused by CCTG repeat expansion in the ZNF9 gene.
Prognosis:
- Congenital conditions can cause early mortality; severity varies.
- With the treatment of respiratory and cardiac diseases, milder variants provide a nearly normal life expectancy.
- The quality of life might be impacted by fatigue, cognitive problems, and multisystem involvement.
CLINICAL FEATURES:
Onset: Adolescent to childhood.
Key symptoms:
- Delayed muscular relaxation, or myotonia.
- Weakness in the distal muscles (hands, feet).
- Ptosis and facial weakness.
- Heart arrhythmias and cataracts.
- Endocrine malfunction (infertility, diabetes).
Genetic causes and inheritance:
- GenesDMPK(DM1),ZNF9(DM2).
- Inheritance: Autosomal dominant.
Prognosis:
- Severity varies; congenital forms may lead to early death.
- Milder forms allow near-normal life expectancy with the management of cardiac and respiratory issues.
- Fatigue, cognitive issues, and multisystem involvement can impact quality of life.
4. Limb Girdle Muscular Dystrophy(LGMD):
LGMD affects the shoulder(scapular) and hip girdle and has autosomal dominant and recessive forms.
CLINICAL FEATURES:
- Onset: Childhood to adulthood(varies by subtype).
Key symptoms:
- Weakness in the shoulders and restricted arm movement.
- Stiffness and contractures in the joints.
- Dysphagia, or difficulty swallowing, in extreme cases.
- Walking with difficulty and falling a lot.
- Progressive weakening of muscles without affecting cognition.
- Some types include respiratory problems and cardiomyopathy.
Genetic cause and inheritance:
- Multiple genes are involved(CAPN3, DYSF, SGCA, etc).
Inheritance:
- Autosomal dominant(LGMD1):milder.
- Autosomal recessive(LGMD2):more severe.
Prognosis:
- While some types cause early ambulation loss, others maintain mobility for many years.
- Lifespan may be severely impacted by cardiac and respiratory issues.
5.Facioscapulohumeral Muscular Dystrophy(FSHD):
FSHD mostly affects the upper arms, shoulders, and face. It develops gradually with stable intervals.
CLINICAL FEATURES:
Onset: Adolescence to early adulthood.
Symptoms:
- Face weakness: trouble smiling, whistling, and closing eyelids.
- Blades of the shoulders protrude in scapular winging.
- Upper arm weakness that spreads to the legs.
- Asymmetry is a prevalent phenomenon.
Genetic causes and inheritance:
- Gene DUX4 gene on chromosome 4.
- Inheritance: Autosomal dominant.
Prognosis:
- Slow progression, usually a regular lifespan.
6.Congenital Muscular Dystrophy(CMD):
A group of early-onset muscular dystrophies, CMD is normally present at birth or within the first year of life. Some subcategories entail cognitive and cerebral dysfunction.
CLINICAL FEATURES:
Key Symptoms:
- Hypotonia and widespread muscular weakness (sometimes known as “floppy baby syndrome”).
- Contractures of the joints (arthrogryposis).
- Delayed motor development.
Genetic Cause and Inheritance:
- Genes:LAMA2(Merosin-deficient CMD),FKRP,POMT1,etc.
- Inheritance: Autosomal recessive.
Prognosis:
- Severe types might cause respiratory failure and early death.
- With supportive care, milder variants might enable survival into maturity.
7. Emery Dreifuss Muscular Dystrophy(EDMD):
Skeletal and cardiac muscles are impacted by EDMD, which frequently results in early-onset heart disease.
CLINICAL FEATURES:
- Onset: Childhood to early adulthood.
Symptoms:
- Early contractures(elbows, Achilles tendons, neck).
- Slow progressive muscle weakness.
- Cardiac conduction defects(arrhythmias, sudden cardiac death).
Genetic Cause and Inheritance:
- Genes: Emerin(EMD gene, X linked), LMNA gene(Autosomal dominant/recessive).
Inheritance:
- X-linked(EMD mutation): More severe in males.
- Autosomal dominant/recessive(LMNA mutation).
Prognosis:
- Muscle weakness progresses gradually, often leading to mobility issues.
- Cardiac complications (arrhythmia, heart failure) are major concerns.
- With pacemaker implantation and respiratory support, life expectancy can be near normal.
8. Oculopharyngeal Muscular Dystrophy:
Oculopharyngeal Muscular Dystrophy (OPMD) is a rare, late-onset genetic condition that mostly affects the ocular muscles, which govern the eyelids. It is characterized by gradual muscle loss. Mobility issues may result from its gradual effects on the limbs and proximal muscles.
Inheritance Pattern:
- Autosomal Dominant(most common): The most prevalent kind, autosomal dominant, is caused by a single mutant copy of the PABPN1 gene from one parent.
- Autosomal Recessive (rare): A more severe version of the disease results from a mutation in both copies of the PABPN1 gene.
Symptoms:
- Ptosis(Drooping eyelids).
- Dysphagia(Difficulty swallowing).
- Proximal Muscle weakness.
- Dysarthria(Speech difficulties).
- Aspiration Pneumonia.
Prognosis:
- Aspiration pneumonia may result from difficulty swallowing.
- Later in life, movement may be impacted by muscle weakness.
- With proper care, life expectancy is often close to normal.
DIAGNOSIS OF MUSCULAR DYSTROPHY:
1. Clinical Evaluation:
A)Medical History:
- Development and progression of symptoms: For example, weak muscles, trouble walking, and Frequent falls.
- History of MD or related neuromuscular conditions in the family.
- Associated symptoms include respiratory disorders, learning disabilities, and cardiac issues.
B)Physical Examination:
- Weakness in the muscles (the pattern of weakness helps identify the kind of MD).
- Abnormalities in gait (e.g., toe walking, waddling gait).
- Either muscle hypertrophy (enlargement) or atrophy (wasting).
- Muscle tone and reflexes shift.
- Gower’s sign: Duchenne muscular dystrophy is frequently accompanied by difficulty getting up from the ground and pushing with the hands on the thighs.
2. Laboratory Tests:
A) Blood test for creatine kinase (CK):
- CK is an enzyme, generated during the breakdown of muscle fibers.
- Although not unique to MD, elevated CK values are indications of muscle injury.
- Aids in distinguishing between neurological and musculoskeletal conditions.
B) Genetic Testing:
- Verifies which gene mutations specifically cause MD.
Techniques consist of:
- Dystrophin gene deletions are detected by PCR (Polymerase Chain Reaction) (Duchenne/Becker MD).
- Multiple Ligation-dependent Probe Amplification, or MLPA: Single nucleotide mutations are detected through Next Generation Sequencing (NGS).
3. Electrophysiological Tests:
A)Electromyography (EMG):
- Assesses muscular electrical activity.
- Distinguishes between nerve and muscle diseases (such as MD).
B) Muscle Biopsy reveals;
- Degeneration and regeneration of muscle fibers.
- Infiltration of fat and fibrosis.
- Dystrophin protein decrease or absence (in Duchenne/Becker MD).
4. Imaging Studies:
- MRI (Magnetic Resonance Imaging): Helpful in distinguishing between different kinds of MD.
- Ultrasound: Without invasive biopsies, ultrasound can identify abnormalities in the muscles.
5. Cardiac and Respiratory Tests:
A) ECG and echocardiogram:
- Assess cardiac function, particularly in Duchenne, Becker, and Emery Dreifuss MD.
B) PFTs (pulmonary function tests):
- Assess lung function, particularly in situations with advanced lung disease.
6. Differential Diagnosis:
MD symptoms may resemble other conditions like:
- Congenital myopathies.
- Spinal Muscular Atrophy(SMA).
- Metabolic myopathies.
- Inflammatory myopathies(eg: Polymyositis, dermatomyositis).
ROLE OF AYURVEDA IN MUSCULAR DYSTROPHY:
Our hospital specializes in a multi-disciplinary approach, bringing together Ayurveda, physiotherapy, and acupuncture for healing. While muscular dystrophy (MD) has no definitive cure, Ayurvedic treatment focuses on symptom relief and slowing its advancement.
Treatments provided in our hospital are,
INTERNAL MEDICATIONS GIVEN ARE:
- Vidaryadi kashayam.
- Dhanwantharam Kashayam.
- Sahacharadi Kashayam.
- Amrthotharam Kashayam.
- Dhanadanayanadi Kashayam.
- Saraswatharishtam.
- Indukantham syrup.
- Shaddharanam tab.
- Nayopayam Kashyam.
- Shadpala Ghrutham.
- Vaiswanara Choornam.
- Ksheerabala 101 avarthi capsule.
EXTERNAL TREATMENTS GIVEN ARE:
DHARA:

Dhara is a unique Ayurvedic Therapy where medicated liquids are poured in a continuous stream over a specific part of the body or entire body. It is widely used in neurological and muscular disorders including Muscular Dystrophy(MD).
There are different types of Dhara. Normally used Dhara in Muscular Dystrophy are:
- Kashaya Dhara: Dashamoola Kashya is used.
- Dhanyamla Dhara: Dhanyamala(A fermented liquid is utilized here).
- Dashamoola Ksheera Dhara: It utilizes a medicated milk(Ksheera) decoction enriched with Dashamoola herbs.
After maintaining a moderate temperature, warm liquids are poured over the specific area/entire body for 30-60 minutes.
Benefits of Dhara:
- It strengthens muscles and delays degeneration.
- It improves neuromuscular coordination.
- It balances Vata Dosha(the chief cause of degeneration).
- It enhances blood circulation and oxygen supply.
- It relieves muscle pain, spasms, and stiffness.
- It detoxifies and rejuvenates the body.
- It provides mental relaxation and reduces stress.
NASYAM:

Nasyam is a specialized Panchakarma therapy in Ayurveda that involves administering medicated oils, herbal extracts, or powders through the nasal passages. It is particularly effective for disorders of the head, brain, and nervous system.
The patients should be given a face massage and steam. The patient lies down with their head tilted backward. Medicated oil or powder is then instilled into the nostrils.
The patient is advised to spit out secretions and avoid cold exposure or heavy meals immediately. Herbal smoking(Haridradi Varthi) should be followed by this procedure.
Two modes of Nasya are normally performed here:
- Marsha Nasyam: It involves administering higher doses of medicinal oil(6-10 drops). Ksheerbala Taila is used.
- Prati Marsha Nasyam: Unlike Marsha Nasyam, it is of minimum dosage(2 drops daily). It is gentle, preventive, and practiced daily to maintain nasal and neurological health. Normally Anu Taila is used for this.
Benefits of Nasya:
- It strengthens the nervous system.
- It balances Vata dosha.
- It improves blood circulation and oxygenation.
- It reduces muscle stiffness and spasms.
- It delays disease progression.
PODI KIZHI:

Podi Kizhi(Choorna Pinda Sweda) is a traditional Ayurvedic Therapy that involves the application of medicinal powders(Herbal Choornam)wrapped in a cloth and heated before being massaged to the body. Kolakulathadi Choornam is usually used and Kizhi is done about 30-45 minutes.
Benefits of Podi Kizhi:
- It improves muscle tone and strength.
- It enhances blood circulation.
- It reduces stiffness and spasticity.
- It aids in pain relief.
- It prevents contracture.
- It supports nerve system function.
NJAVARA KIZHI:

Njavara Kizhi(Shashtika Shali Pinda Sweda)is a specialized Ayurvedic Treatment involving the massaging of heated medicinal rice poultice to the body. It is highly effective in managing neuromuscular and musculoskeletal disorders. Normally half to one-hour sessions of Kizhi are done.
Benefits of Njavara Kizhi:
- It helps in muscle strengthening and nourishing.
- It improves blood circulation and oxygenation.
- It balances Vata Dosha.
- It enhances nerve function and coordination.
- It increases flexibility and reduces stiffness.
- It delays the progression of the disease.
ELA KIZHI:

Ela Kizhi is a Swedana(Sudation therapy) where medicinal leaves are fried with medicinal oils and tied into boluses(Kizhi). These boluses are heated and massaged over the body to induce perspiration. Castor leaves(Eranda, Ricinus communis), Tamarind leaves(Tamarindus indica), Arka leaves(Calotropis gigantea), etc are generally used to make Elakizhi.Dhanwantharam Thailam, Pinda Thailam, and MahaMasha Thailam are normally used in Muscular Dystrophy.
Benefits of Ela Kizhi:
- It improves blood circulation and muscle nutrition.
- It strengthens weak muscles and nerves.
- It pacifies Vata Dosha.
- It pacifies stiffness.
- It enhances neuromuscular coordination and movement.
- It increases flexibility and reduces muscle spasms.
- It slows down the disease progression.
ABHYANGAM:

Abhyanga is a traditional Ayurvedic Oil massage that nourishes, strengthens, and rejuvenates the body. It is a vital therapy in musculoskeletal disorders like Muscular Dystrophy. The medicated oil was chosen based on the individual’s Dosha(body constitution) and disease condition. The oil is warmed and used. Usually, Dhanwantharam Thailam, Pinda Thailam, and MahaMasha Thailam give results in this condition. The massage is done about 30-60 minutes. The patient is advised to rest for 15-30 minutes for oil absorption. A warm steam therapy is given to enhance relaxation.
Benefits of Abhyanga:
- It nourishes and strengthens muscles.
- It improves blood circulation and oxygenation.
- It pacifies Vata Dosha.
- It enhances neuromuscular coordination.
- It improves joint mobility and reduces stiffness.
- It removes toxins and enhances detoxification.
ROLE OF PHYSIOTHERAPY IN MUSCULAR DYSTROPHY:
Physiotherapy plays a crucial role in managing muscular dystrophy.
Range of Motion Exercises:
A)Passive Range of Motion(PROM) Exercises:
- Here the therapist moves the joint of the patient passively.
B)Active Assisted Range of Motion:
- Here the patient moves the joint with some assistance.
C)Active Range of Motion(AROM):
- Here the patient moves the joint without any assistance.
ROM Exercise:
1. Neck ROM exercises:
- Neck flexion and extension.
- Neck side bending.
- Neck rotation.
2. Shoulder and Arm ROM:
- Shoulder flexion and extension.
- Shoulder abduction and adduction.
- Elbow flexion and extension.
3. Wrist and Hand ROM:
- Wrist flexion and extension.
- Knee bending and straightening.
4. Ankle and Foot ROM:
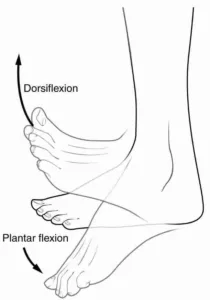
- Ankle dorsiflexion and Plantar flexion.
- Toe flexion and extension.
Strengthening Exercises:
A)Isometric Exercises(Static Strengthening):
- It reduces strain by contracting muscles without moving.
Examples:
- Seated knee extension.
- Pressing a hand against the wall.
- Abdominal bracing(Core strengthening).
B)Low Resistance Dynamic Exercises(Active Movement):
- Controlled movement with minimal resistance.
Examples:
- Seated leg lifts.
- Arm raises with light weights.
- Mini squats with support.
C)Functional Strengthening:
- Helps the patient perform daily activities.
Examples:
- Sit to Stand exercises.
- Stair stepping(with support).
- Assisted walking exercises.
Assistive Devices and Orthotics:
- Individuals can continue to move, carry out daily tasks, and lessen the impact on weak muscles with the assistive equipment.
Mobility Aids:

- Canes and walking Sticks.
- Forearm crutches and armpit crutches.
- Walkers.
- Wheelchairs.
Orthotic Devices in Muscular Dystrophy:

- Ankle Foot Orthosis.(AFO).
- Knee Ankle Foot Orthosis(KAFO).
- Spinal Braces.
- Hand and Wrist splint.
Electrotherapy:
A) Transcutaneous Electrical Nerve Stimulation (TENS):

- This technique modulates pain signals and enhances circulation by passing low-voltage electrical currents through the skin.
B) Ultrasound:

- It improves healing and lowers inflammation by penetrating deep tissues with high-frequency sound waves.
Gait Training and Balancing Therapy:
- The goals of gait training are to increase endurance, decrease compensatory movements, and improve walking patterns.
a)Strengthening and stretching:
- Target muscles: Hip flexors, glutes, quadriceps, and core.
Examples:
- Bridging exercises.
- Leg lifts.
- Resistance and exercises.
- Ankle and toe exercises.
b)Walking Pattern Correction:
Examples:
- Split squats
- Leg swings
- High knee lifts,
- Toe walks
- Step over
c)Static and dynamic balance exercises:
- Standing on one leg.
- Tandem walking.
- Balance board exercises.
- Obstacle walking and uneven walking to enhance proprioception.
Vestibular and Proprioceptive training:
Vestibular exercises for head and eye coordination.
- Move the head up and down and side to side while maintaining focus on a stationary item.
- Go slowly at first, then speed up the pace.
Target tracking:
- Move eyes to follow a moving object without moving the head.
- It helps improve coordination between vision and balance.
Vestibular adaptation and habituation exercises:
- Closing their eyes and marching in a single spot.
- Gently making circles while keeping your attention on a single target.
- Walking while turning your head up, down, and side to side.
Benefits of Physiotherapy in Muscular Dystrophy:
- It maintains muscle strength and function.
- It improves mobility and flexibility.
- It enhances posture and reduces pain.
- It supports breathing and lung function.
- It improves balance and reduces falls.
- It promotes independence and well-being.
DIET RECOMMENDATIONS IN OUR HOSPITAL:
Our senior physicians suggest to avoid:
- Milk, milk products, cold food, pickles, fruits, dry fruits, nuts, fast food, fried and oily foods.
- Fermented foods like dosa, idli, and fermented appam.
- Tuber items like potato, tapioca, and sweet potato.
- Nonvegetarian items like Fish, egg, and meat(Can be taken in curry form, if necessary).
A few recommended food items to be taken are:
- Hot kanji.
- Steamed food items like idiyappam, put, and chapati.
- Vegetable in boiled form.
General Suggestion:
- Avoid strenuous activities.
- Drink enough water(2.5L-3L).
DISCLAIMER: The information provided in this article is intended solely for educational purposes. Treatment decisions should be made exclusively by a well-qualified Ayurvedic physician. Self-medication is strongly discouraged.
Maurya Ayurveda Hospital,opposite to Sabine Hospital,Pezhakkapilly P.O,Muvattupuzha,Ernakulam;PIN:686673,Contact no:9947183000
Email: info@mauryaayurveda.com
Maurya Ayurveda Ortho & Neuro Rehabilitation Centre ( Ayurveda Hospital )